Nigeria has low brain awareness
Summary
Prof. Mustapha Danesi: "Social attitudes impede effective treatment of brain diseases, which are usually attributed to something mysterious."
Prof. Mustapha Abudu Danesi, Consultant Neurologist, College of Medicine, University of Lagos, had his Inaugural Lecture, entitled: “The African Brain: Effects of African Environment on Brain Diseases,” last month. He spoke with Jide Akintunde and Martins Hile, editors at Financial Nigeria Magazine, after the Lecture.
Financial Nigeria Editors: Congratulations on your Inaugural Lecture which was delivered on August 05, 2015 at the Main Auditorium of University of Lagos. One of the conclusions you drew was that the physical and social conditions of Africa exerts contradictory influences on brain diseases in sub Saharan Africa. How is this the case?
Mustapha Danesi: The social environment in sub-Saharan Africa has an adverse effect on brain diseases. In my Inaugural Lecture, I used epilepsy as a major example. I also used tetanus, HIV and stroke. Starting with epilepsy, you find out that the beliefs and attitudes of the public towards epilepsy has a serious negative effect on people with this disease. It stigmatizes them; and as a result of that, they have a lot of psychological and social problems.
For example, people believe that epilepsy is infectious so they shun epileptic patients. Schools dismiss them and employers refuse to hire them once they know they are epileptic. Due to such stigmatization, epileptic patients sometimes don't want to accept that they have the disease. This has a serious effect on the management of the disease.
When they hide their conditions, they end up doing jobs that are dangerous. For example, you see an epileptic patient driving a taxi or a bus. If he has an attack while driving, he will have a fatal accident. And because our social environment is mystically oriented, we feel that epilepsy is caused by evil spirits. As a result, epileptic patients fail to seek medical treatment; they go to traditional practitioners or seek spiritual healing. They believe these are the people that would be able to take care of what is causing their epilepsy.
A lot of them go into these ineffective treatments for a long time. Sometimes, we see epileptic patients who, for the past five years, have been going from one traditional practitioner to the other. Eventually they stumble into the hospital. When we start giving them medication and their seizures get controlled, they are surprised.
Their social environment is what discourages them from seeking orthodox medical treatment because of the belief that it is caused by evil spirits and witchcraft. This mystical orientation in our social environment affects the disease and its management.
The treatment gap for epilepsy is very wide. You find out that about 70-80 per cent of people with epilepsy in Nigeria today do not seek medical treatment because they are stuck in the rural areas where anti-epileptic drugs are not available at the primary healthcare centres. Even those who are able to afford medical treatment pay from their pockets because there is no coverage of health insurance.
This treatment is not like malaria whereby you buy a drug and you are cured. This is a life-long treatment. You have to take the drug all the time. You find that after buying the drug over a period of one or two months, a lot of them cannot afford to continue to take the drug regularly. As a result of that, their seizures are not controlled. In my research, I found that only 36 per cent of our patients are controlled; whereas, in the developed world, up to 75 per cent of cases usually get controlled because they take their drugs regularly.
Where there is good medical care, epilepsy in not common. Epilepsy is more common in our environment than in the developed world. Even in our own environment, when you go to rural areas where medical care if nonexistent, you find out that epilepsy is rampant. A lot of the children are born with birth asphyxia. As a result, most of them are always convulsing because they are not immunized. Our social environment not only encourages epilepsy, it also discourages effective management of the condition.
It is easy to eliminate a condition like tetanus. In advanced countries, tetanus is virtually unknown. When I was working in Virginia, there was one tetanus case in Chicago. They called me and I had to manage the tetanus patient over the phone from Virginia because the doctors there didn't know how to manage it. They may have one tetanus case in three years. But if you came to our ward here, you would find two or three patients on admission with tetanus. It is so rampant here because most adults have not been immunized against tetanus. Here also, our social environment has been very poor in eliminating tetanus.
The same thing with HIV. It is very uncommon to see brain disease as a result of HIV in advanced countries. However, here in Africa, brain diseases are the commonest manifestation of HIV. Up to 58 percent of people with HIV in Africa have brain diseases. When you treat HIV and reduce the viral load, the brain escapes manifestation. But when they are not treated, the brain is one of the first port of call. The reason they are not treated is that most patients don't know they have HIV, especially because of the stigma attached to it. So voluntary testing and counselling does not occur.
Once we improve our social environment and treat every patient coming with HIV, we would be able to eliminate this neurological condition.
Stroke is the commonest complication from hypertension cases in Africa. We have rampant cases of stroke here because we do not know how to prevent it. In the epidemiology that we did, it showed that age-adjusted incidence of stroke in Nigeria is similar to the incidence in France. Whereas, about 30 years ago, the incidence of stroke in France was three times what we had in Nigeria. This means that while the incidence has been reducing in France, here it has been increasing. The reason is that we do not address the issue of prevention. The population is not aware of the risk factors for stroke so they don't know how to avoid it. So it's a challenge to our social environment to look at how to prevent stroke by addressing the risk factors.
Apart from hypertension, the other risk factors for stroke are smoking, diabetes mellitus and poor nutrition. Stroke is more common among poor people who are malnourished. Many of them would have infection or hypertension and they wouldn't know. So our social environment encourages stroke to occur. These are challenges we need to address.
There is also high stroke mortality because we don't have enough manpower that is knowledgeable enough to handle the condition. It is a challenge to neurologists to teach doctors how to manage stroke so that we can reduce the incidence. Because our social environment is still very ignorant, a lot of neurological conditions cannot be treated effectively.
On the positive side, the physical environment is very protective of the brain. The high environmental sunshine has now been proven to protect the brain. My seminal work had earlier shown that for people who expose themselves to high environmental sunshine, their brains are not as excitable as patients who do not have the exposure to sunshine. For example, a lot of epileptic patients in Europe have seizures when they are watching TV, playing video games or at the disco because of the flickers of light.
However, we are protected against that in this environment because the sunshine has stabilized our brains to the extent that such triggers don't affect us. Of course I had demonstrated that in the laboratory. Initially, we didn't know the reason. We used to attribute it to noradrenaline and dapomine but recently it's been shown that vitamin D has protective effects on the brain. It reduces excitability of the brain and this protects against epilepsy. Vitamin D is known to protect against a range of brain diseases so the severity that is usually associated with these diseases is not here. I can appreciate this acutely because I have practiced in Europe and the United States, and I practice in Nigeria. The type of severity we see in diseases like migraine, Parkinson’s and dementia does not occur here. In the United States, there is no time you don't have epileptic patients on admission because of crisis of seizures. But in the past one of two years, there has been none in our ward here.
Even status epilepticus, epileptic cases that come in as an emergency, is so common in Europe that you can't go for a single day without having one. In the past one and half years, we have only had three in LUTH. The manifestation of our neurological diseases is much more benign as a result of the protection from sunlight.
I have proved this protection because of the work I did looking at summer and winter patients in the UK and I have been able to prove that in the summer, when there is a lot of environmental sunshine, the brain is more stable among British epileptic patients. Their photoparoxysmal discharge is less. Whereas, in winter, that excitability is increased which I have proven in my work when I was in Institute of Neurology, Queens Square, London.
Our physical environment protects the brain; whereas our social environment has an adverse effect on brain diseases.
FN Editors: You also drew an evidence-based conclusion on the relative resilience of the people of the sub-continent to certain neurological conditions, compared to data from your survey in Britain; and you said the disparity is not genetic but climatic. Providing more insights into this, how can we maximize the tropical advantage in reducing brain diseases?
MD: The tropical environment helps protect the brain. Initially, people thought it was genetic endowment but I have proven that it is not. Black people in Europe and America have as much severe brain diseases as white people. So even in my practice, I have found no difference between racial groups in the severity of neurological diseases in America or Europe. It is the environment that protects the brain here.
I can answer your question by drawing analogies from experiences in other parts of the world. That analogy might be able to give you an indirect answer. For example, in a disease like multiple sclerosis, when they looked at people's occupation in the United States, it was discovered that people with multiple sclerosis whose occupation expose them to the sun usually have mild cases of the disease, compared to people whose occupation keeps them indoors. Exposing themselves to sunshine reduces the severity of the disease. Again this was attributed to high vitamin D level.
In another study of dementia patients, one group was exposed to the sun. They were taken outside every day and exposed to the sun. Another group was managed in the traditional way they manage them in nursing home. After sometime, they found out that the group that was taken outdoors improved dramatically and their outlook was better. The group that was kept indoors did not improve as much as the other group. This showed that exposing this group of people to the sun actually improved their brain condition.
Looking at these two analogies, we found out that in order to maximize this tropical advantage, we need to try to expose ourselves more often to the sun. Some people whose occupation keeps them indoors at all times and they don't get exposed to the sun – if they do develop these conditions – run the hazard of having a more serious brain condition like Parkinson or dementia.
If you take a 30-40 minute walk when the sun has risen, it is more beneficial than taking a 30-minite walk at night time. Exposing ourselves to the sun will maximize the benefit of the sun in protecting our brain.
FN Editors: We also noted that you ascribe certain effectiveness to spiritual activities in the management of such conditions like epilepsy. Would you like to put this in perspective?
MD: As I said in my lecture, spiritual healing, even though it is ineffective in controlling seizures, it is still being used by quite a number of people. The reason is that there are certain things they benefit from spiritual healing we cannot give. For example, apart from the seizure, epileptic patients suffer a lot of psychological stress conditions. They are depressed; they have fears etc. In advanced countries, they meet with traditional psychotherapists who give them psychological treatments, counseling and so on in order to balance the medical treatment we give.
In this part of the world, however, psychotherapy is not that effective because we are living in a social environment that has mystical orientation. An epileptic patient thinks there are mystical forces that brought him the disease. We have no way of giving psychotherapy that will erase that from his mind. So when the spiritual healers now talk about these spiritual forces that are disturbing him, they feel confident that these people have the capacity to deal with their problem.
Somebody has told me, “Doctor, you can give me drugs to suppress this seizures but why am I the only one in my entire family who has this condition? Don't you think that some evil forces brought it to me? You don't have the capacity to remove those evil forces but there is someone who can. So I will have to consult that person.” In our mystically-oriented environment, traditional psychotherapy does not work so well but spiritualists are very effective in addressing the psychology of our people. That is why churches are booming because they address the spiritual needs.
A lot of our epileptic patients are like this and I don't discourage them. I believe the psychotherapy we offer cannot address their psychological and spiritual needs. But I have to also advise them to take my prescription. That is the way to balance it because of our social environment.
FN Editors: Yet, again, you made an interesting but alarming disclosure that Africans tend to use more of the right hemisphere of the brain, which is responsible for the expressive arts, than the left hemisphere of the brain which is responsible for, amongst other things, scientific innovations. Is that who we are as Africans or it is who we are been conditioned to be?
MD: There is still a big research question in this area that needs to be looked into. But of course I had said that the right brain is the brain for artists, and the left brain is the brain for scientists.
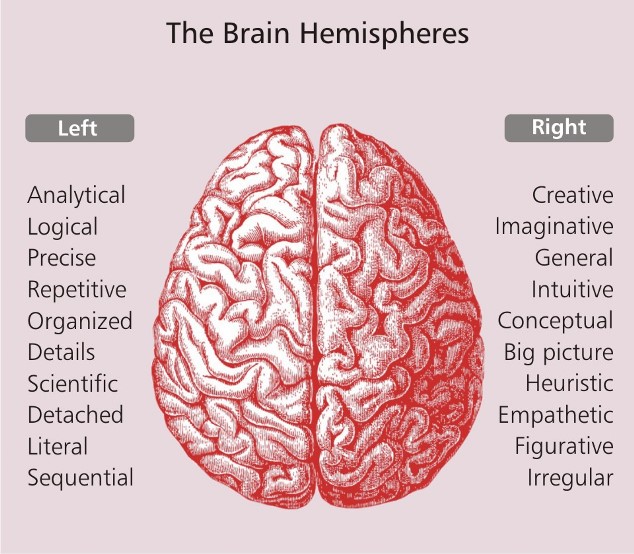
A scientist is someone who carries a torchlight in the dark, searching for hidden truth in nature. And whenever he finds that truth, he expresses it in form of scientific discovery. A lot of the time it needs collaborators. That is why a scientific paper sometimes has many authors because each one looks at various aspects. You find that scientific discoveries are cumulative.
There is nothing a scientist makes. God has already provided these things. It's just a question of discovering God's law in nature. The artist is not concerned about truth in nature. He is interested in the realities of the environment. To put it in perspective, an artist carries a mirror that reflects accurately the realities of our social and physical environment in forms of dramatic arts, painting, music etc. The artist is not concerned with scientific truth.
So the two hemispheres of the brain serve different functions. Music appreciation is the right brain function. A very good artist is also good in music because it is all a function of the right brain.
Does our social environment make us carry a mirror more in expressing or does it make us look at the hidden truth in nature? Although we still need to investigate this properly, from my investigation, our social environment conditions us to look at the realities. For example, in our folklore, we have a lot of festivities where music and dancing are part of that culture. So our brain develops along that pathway because our folklore encourages festivities, music and dancing. Then you look at our mystically-oriented society. In our belief systems, we always think of our ancestors, whatever they did, we want to replicate it. That is not scientific because some of those beliefs might have been obsolete. And then you are asked to believe in something, whether it makes logical sense or not. If it is your elder that says you must believe in this or that, you can't question it.
We believe so much in what our ancestors did. Whereas, the left brain is not attuned to that. It is the logical part of the brain. Anything that does not make logical sense is discarded. Our culture doesn't allow us to do that. There are still many things we are asked to take and believe in that don't make logical sense. But that is part of our social environment.
Until we discard that culture that says we can't question our elders and our ancestors, then we will never encourage our brain to think critically and logically. So the social environment does not allow for the left brain to develop. The left brain is logical, it upends the status quo. In essence, our social environment allows for the development of the right brain and suppresses the expression of the left brain so that scientific expression is not encouraged. If you want to develop a scientific mind to question some of the things that occur, you will end up being called a rebel.
But you cannot say the white man's brain is superior to the black man's brain. For example, while the white man might have had some scientific innovations because his environment encourages critical and scientific thinking, the black man's brain has also contributed something profound to the world. In the world of art, you will find works of art from Africa in museums all over the world. Black people have won laurels and excelled in other areas.
FN Editors: Patients of neurological conditions still have to engage the work and study environments. How do social attitudes reinforce what might be poor treatment outcomes of brain diseases in sub Saharan Africa and what could be possible remedies?
MD: I have already said our social attitudes would reinforce poor treatment outcome. For example, we go to traditional practitioners instead of using orthodox medicine. Our neighbours are more influential in determining our health-seeking behaviours than even our general practitioners. What the neighbours tell you is what you are likely to take. As a result, social attitudes impede effective treatment of brain diseases, which are usually attributed to something mysterious. Until our social attitudes improve, we are always going to have these diseases. The remedy is that Africans need to understand the brain more. If we don't, we will continue to attribute brain diseases to mysticism.
FN Editors: More generally, what is the state of the practice of neurology in Nigeria and what do you consider as the more important contributions you have made to it?
MD: Today, neurology is getting better. We have close to 70 people who are neurologists in Nigeria.
I left for the U.S. in 1996. I had a four-year contract, a direct employment. The contract was to lead to some bigger position. In fact, they had asked me if I needed a green card. I said I didn't because I wanted to watch the situation. I wasn't so sure if I wanted to run away from my country as a result of the economic hardship here in the 1990s.
At that time, there were only seven neurologists in Nigeria. In the entire north, there was only one psychiatrist, who also called himself a neuro-psychiatrist. He was based in Kano. There was only one neurologist in the east and the other five were in the west.
One of the factors that made me return to Nigeria in 1998 was that I discovered there were 16,000 neurologists in the United States. There were only seven practicing in Nigeria. What role was I going to play in a society that already had 16,000 neurologists? I will have very little impact. So I felt I needed to come back to Nigeria to develop neurology. The state of neurological practice was abysmal. So I decided to come back without even finishing the four-year contract. They asked me why I wanted to come back and I told them I wanted to develop neurology in my country. So when I came back, they gave me materials that I needed, especially the curriculum of the American Board of Psychiatry and Neurology. They also advised me on what I could do to develop neurology in the country.
I also had the curriculum for training neurologists at the Institute of Neurology, University of London, which is the foremost neurology institute in the world. I combined these two syllabi, studied them critically and drew up a 27-page document on training neurologists in Nigeria. I was chairman of the neurology committee of the National Post-Graduate Medical College. Together with my colleagues on the committee, we got the document ready and submitted it to the National Post Graduate Medical College Senate. They looked at it, vetted and approved it in 1999. So it became the first curriculum for training neurologists in the country. We started to use it in 2000.
It is now the curriculum for training neurologists in the West African sub region. It was adopted five years ago. Most of the neurologists we have trained using that document have proven their mettle. We have very renowned people who have passed through our system.
FN Editors: When one considers the deliberate patriotic choices you have had to make with your career, coming to work in Nigeria as against remaining abroad to earn more and, perhaps, have more fame, one would tend to be piqued with doctors in Nigeria today who regularly abandon their patients because of wage disputes. Well, as an activist yourself, what is the socio-political context to the low level of access to quality medical care in Nigeria?
MD: I will look at this from two perspectives: The government's medical arrangement perspective and the providers' perspective. I have often said the medical profession is so disorganized that it needs a lot of input to get the system back on track. Any doctor who comes to Nigeria and wants to set up medical practice business will soon find out it is not a viable business in Nigeria. As a result, it discourages a lot of doctors from the diaspora from coming to set up medical care as a business. The medical financing system in Nigeria is very wrong and does not encourage medicine to develop. The health insurance is known all over the world as the financing system that makes medical care viable. In the U.S., you contribute a small amount to a private health insurance system and they take care of your health needs. But here in Nigeria people still pay from their pockets. A viable health insurance system would have taken care of everybody in this country and healthcare would have been a viable business.
So you have a situation where people rush to government hospitals because they have no money to pay for private hospitals. The health financing system is such that government still bears the burden. But if we had a good health insurance system that covers everybody, then that system would organized in a way that everybody will have access. I have often said, it is not free healthcare that we need; we need good financing system that will allow everybody equal access to healthcare. That is the problem on the government's side.
On the doctors' side, you find out that because of the system in place, there is a poor attitude in our younger doctors. Many of them look at medical practice as an endeavour to make money. They don't see it beyond earning a living. We have the Hippocratic oath that is given to medical doctors when they graduate. I doubt if they read those documents. You find that a lot of doctors really need to be retrained on medical ethics. It's a challenge that has to be taken up.
A lot of doctors don't even know the legal aspects of medical practice. They need to be retrained on medical laws and jurisprudence. They need to know what their responsibilities and privileges are so they don't fall foul of medical laws.
Apart from earning a living, they need to know they are providing services that are vital. And when they provide these services, not only do they earn a living, they also earn the respect of society. The money aspect is what is more emphasized than the responsibility aspect which is what will earn them the respect of the public.
FN Editors: What do you plan to do to provide wider access to your inaugural lecture which, we believe, would benefit students and professionals in medicine as well as the general public?
MD: For now, there is what I call brain “illiteracy” or very low brain awareness. The brain is the only organ we use. We are not aware of our heart, or liver. But we are aware of our brain and we actually use our brain. So we should really be interested in how it works.
In the U.S., brain awareness is high and neuroscience is taught in secondary schools. A secondary school leaver already knows how the brain works. And there are courses on neuroscience that are taught at undergraduate level. So the mysticism attributed to brain diseases is not there in that society.
The Nigerians need to know that they should be aware of their brains and try to know how the brain works. That is very important.
We are going to promote brain awareness among the general public. We will soon launch a website, Africanbrain.org, whose mission will be to promote brain awareness. It will serve a very good purpose for our population to start understanding the brain function. Gradually, it will improve the outlook on brain diseases.
For the practitioners, it is not possible for 70 neurologists to treat 160 million people. So we have to systematically develop a way of implementing continuous professional development of our general practitioners to understand how to treat brain diseases so that they would be useful as the first port of call when someone has a brain disease. We will work on updating the knowledge of practitioners by giving them more knowledge about brain diseases.
As far as the students are concerned, we are increasingly introducing neurology into the curriculum of our undergraduate.

Recent Interviews










Latest Blogs
- CBN is fighting inflation instead of stagflation
- Why electricity privatization failed (2)
- How net metering can boost embedded power generation
- Adaora Umeoji and gender in Nigerian banking leadership
- Is protest an endangered human right of Nigerians?
Latest News
- CBN increases capital requirements of banks, gives 24 months for compliance
- IFC, partners back Indorama in Nigeria with $1.25 billion for ...
- Univercells signs MoU with FG on biopharmaceutical development in Nigeria
- CBN settles backlog of foreign exchange obligations
- Ali Pate to deliver keynote speech at NDFF 2024 Conference